
What Is an Abnormal Mammogram?
An abnormal mammogram means the radiologist saw an area on your breast images that needs a closer look. This could be a mass, a cluster of tiny calcium deposits (calcifications), an area of distortion, or simply an asymmetry between your two breasts. Importantly, “abnormal” does not equal “cancer.” It is a signal that the picture isn’t fully clear yet.
After a single screening mammogram, the most severe categories are rarely assigned right away. Instead, the radiologist often requests additional imaging before deciding on next steps. Dense breast tissue, overlapping structures, or the absence of older images for comparison can all make an area look uncertain on a first read.
Think of it like a photographer asking to retake a slightly blurry photo. The goal is clarity, not alarm. Getting recalled is a normal, built-in part of the screening process designed to catch concerns early while sorting out the many harmless findings.
If findings are complex, using AI PACs Mammogram Second Opinion Online Service can provide additional reassurance and expert review.
How Common Is a Callback?
If you have been recalled, you are in very large company. About 1 in 10 mammograms result in a callback, and the most important thing is not to panic.
The reassuring news is what happens next for most women. Of mammograms initially scored as needing more imaging, most—around 71.5%—resolve to a negative or benign reading after further evaluation. Callbacks are also more frequent on your first mammogram, simply because there are no prior images to compare against.
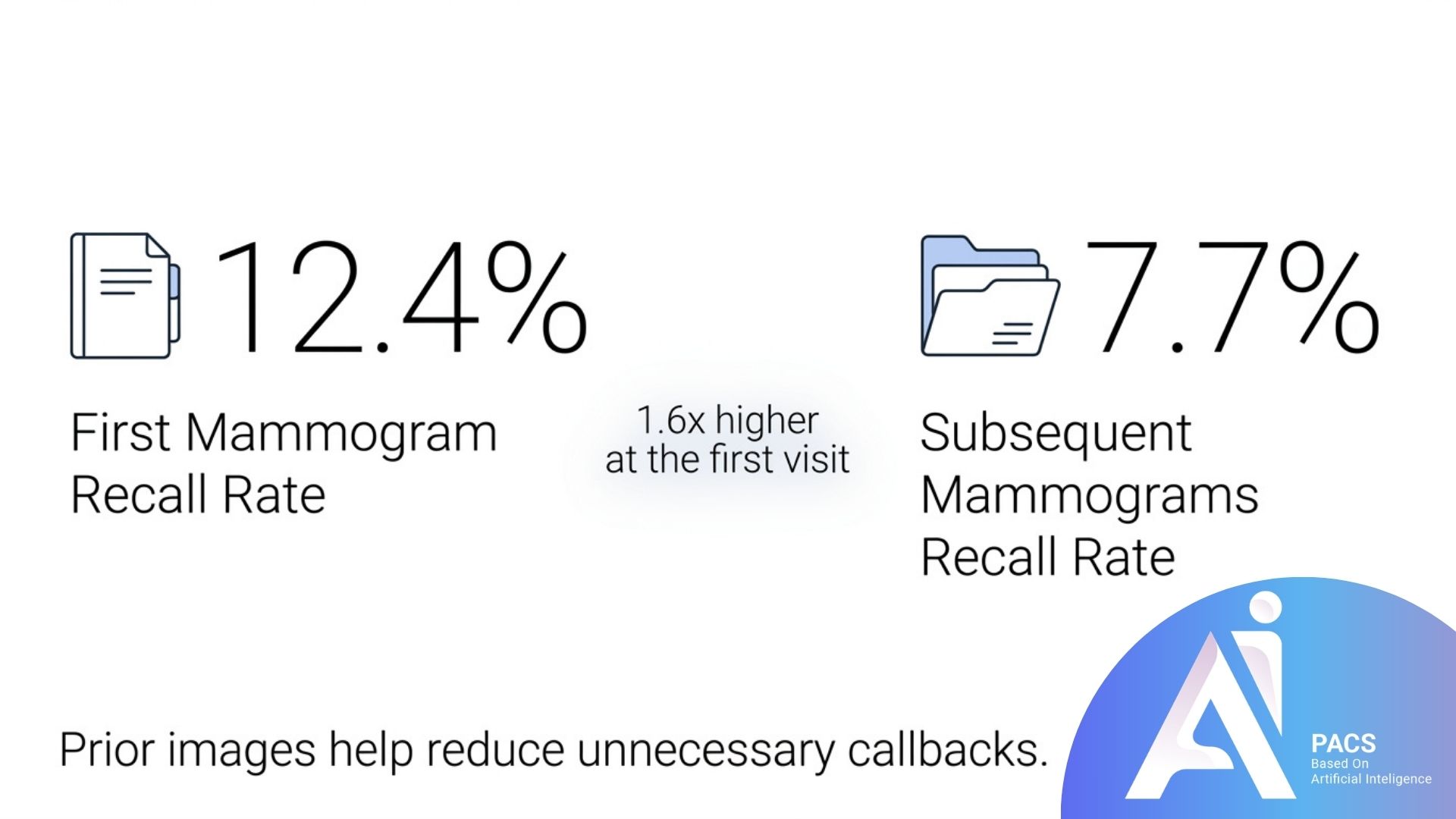
In one large 2023–2024 screening audit, recall rates were 12.4% at a first mammogram versus 7.7% at subsequent mammograms—about 1.6 times higher at the first visit. This is why having prior images available genuinely helps reduce unnecessary callbacks.
Understanding Your BI-RADS Score
Radiologists describe mammogram results using a standardized scale called BI-RADS (Breast Imaging Reporting and Data System). Knowing your number helps you understand exactly what your abnormal mammogram means and what to expect next.
BI-RADS 0 — Incomplete (Needs More Imaging)
A BI-RADS 0 result is the most common reason for a callback. It means additional images—a diagnostic mammogram—are needed before a final assessment can be made. This is the category most often behind the word “abnormal” on a screening report.
BI-RADS 3 — Probably Benign
A Category 3 finding has less than a 2% chance of being cancer but warrants a prompt follow-up, typically a repeat mammogram in six months. If the area stays stable over time, routine screening can resume.
BI-RADS 4 and 5 — Suspicious
Categories 4 and 5 indicate an abnormality where a biopsy is recommended. Category 4 is further divided into subcategories reflecting a range of likelihood, and even here, many biopsies turn out benign.
Read for more information: What Does BIRADS Mean in Mammography?
What Tests Come Next?
Once you are recalled, your care team will tailor the next steps to what they saw. Here is what typically happens.
Diagnostic Mammogram
This is a more detailed mammogram focused on the area of concern. A follow-up diagnostic mammogram with spot compression views is often ordered, frequently alongside a diagnostic ultrasound, to clarify the finding. The result is then resolved into a clear category.
Breast Ultrasound
Ultrasound uses sound waves to distinguish between a fluid-filled cyst (almost always harmless) and a solid mass. It is painless, involves no radiation, and is especially useful in dense breast tissue.
Breast MRI
In selected cases—such as high-risk patients or unclear findings—an MRI provides highly detailed images. The same BI-RADS categories apply, though the recommended next steps may differ slightly.
Biopsy
If imaging still raises concern, a biopsy removes a small tissue sample for examination. For non-palpable lesions found on a mammogram, a core needle biopsy is preferred over fine-needle aspiration because it obtains more tissue for diagnosis. A biopsy is the only way to know definitively, and most results are reassuring.
How to Prepare and What to Expect
Preparing for your follow-up appointment can make the experience smoother and less stressful. A little planning goes a long way.
Bring any prior mammogram images or know where they were done, since comparison films are invaluable. The availability of comparison films roughly halves the odds of a false-positive recall on subsequent exams. Wear a two-piece outfit so you only need to undress from the waist up, and skip deodorant, powder, or lotion on the day of imaging, as these can interfere with the pictures.
It is also wise to sort out logistics early. Contacting your insurance provider before a diagnostic appointment helps you understand expected out-of-pocket costs, and many imaging centers have financial counselors who can help navigate questions or assistance options. Finally, consider bringing a trusted friend or family member for support.

Why Acting Promptly Matters
Scheduling your follow-up sooner rather than later is one of the most helpful things you can do—both medically and emotionally. The waiting period is often the hardest part, and prompt testing shortens it.
In a large National Mammography Database analysis, the median time from an abnormal screening to diagnostic evaluation was just 9 days, and follow-up was documented in 66.4% of abnormal mammograms. This tells us that timely resolution is both achievable and the norm at many centers.
Returning quickly also protects your peace of mind. As one radiologist describes it, relief comes when patients learn their diagnostic mammogram is normal—which is most often the case—and the sooner a patient returns, the better, since lingering anxiety fades once answers arrive.
Latest Scientific Findings
Research continues to refine how we understand and manage abnormal mammograms. Here are several recent, relevant findings.
A 2024 study in the Journal of the American College of Radiology examined nearly 2.9 million abnormal screening mammograms and found meaningful variation in how quickly women complete follow-up. Among recalled mammograms recommended for biopsy, 74.8% of biopsies were documented, with a median time of 21 days from diagnostic evaluation to biopsy. The takeaway: timely follow-up is common but can be improved for some groups.
A 2024 Breast Cancer Surveillance Consortium study, published in the Annals of Internal Medicine, analyzed over 3.5 million mammograms. It found that after 10 years of annual screening, 50–60% of women can expect at least one false-positive recall, and 7–12% will have a benign biopsy—rates that are nearly halved with screening every two years instead. This underscores how common, and usually harmless, recalls are.
Regarding calcifications specifically, a long-term five-year follow-up study of women recalled for calcifications found that the majority of lesions—81.3%—were completely benign. This is reassuring for the many women called back for this exact reason.
Finally, modern technology is reducing unnecessary callbacks. 3D mammography (tomosynthesis) means fewer people need to be called back while also catching more cancers.
Conclusion
An abnormal mammogram is a request for clarity, not a diagnosis. The vast majority of callbacks lead to normal or benign results, and the structured BI-RADS system ensures your care team knows exactly how to proceed. By understanding your score, preparing for follow-up imaging, and acting promptly, you put yourself in the strongest position—both medically and emotionally.
If you have received an abnormal result, the most empowering step is to schedule your follow-up appointment and ask your care team any questions you have. You may also find it reassuring to seek a second opinion on your imaging for added confidence. Please speak with your physician about your specific BI-RADS findings and the next steps that are right for you.
Scientific References
- Oluyemi ET, Grimm LJ, Goldman L, et al. Rate and Timeliness of Diagnostic Evaluation and Biopsy After Recall From Screening Mammography in the National Mammography Database. J Am Coll Radiol. 2024;21(3):427-438. doi:10.1016/j.jacr.2023.09.002
- Ho TH, Bissell MCS, Kerlikowske K, et al. Cumulative Probability of False-Positive Results After 10 Years of Screening With Digital Breast Tomosynthesis vs Digital Mammography. Annals of Internal Medicine. 2024. (Breast Cancer Surveillance Consortium)
- American Cancer Society. Understanding Your Mammogram Report.
- Johns Hopkins Medicine. Understanding Your Mammogram Report.
- Cleveland Clinic. BI-RADS (Breast Imaging-Reporting & Data System). Last updated 10/23/2024.
- D’Orsi CJ, Sickles EA, Mendelson EB, Morris EA, et al. (Eds). ACR BI-RADS Atlas, Breast Imaging Reporting and Data System. American College of Radiology, 2013.
- Silva LSF, et al. Subsequent mammography reduces recall and increases breast cancer detection: an audit of a screening program. NCBI PMC12671671.
- Tan KP, et al. Microcalcifications Detected as an Abnormality on Screening Mammography: Outcomes and Follow-up Over a Five-Year Period. NCBI PMC3806370.
- Breast Cancer Surveillance Consortium. False-Positive Results and Return to Screening Mammography. Sep 2024.
- RadiologyInfo.org. Mammography.
- National Cancer Institute (NIH). Mammograms Fact Sheet.
- U.S. FDA. Mammography: What You Need to Know.