Key Takeaways
- Yes — CT is the first-line imaging test for pancreatic cancer, detecting roughly 85–95% of tumors when a dedicated “pancreatic protocol” CT is used.
- Not all CT scans are equal. A routine abdominal CT can miss small tumors; a multiphase contrast-enhanced pancreatic protocol CT is the standard of care.
- Small tumors under 2 cm are the hardest to see — up to 10–15% may be invisible or subtle on CT, which is why symptoms should never be dismissed by one normal scan.
- CT does more than detect — it stages the tumor, maps blood vessel involvement, and determines whether surgery is possible.
- A second opinion matters. Vascular involvement and small lesions are frequently reinterpreted, sometimes changing a patient from “inoperable” to “operable.
What Is a CT Scan of the Pancreas?
A CT (computed tomography) scan uses X-rays taken from many angles around your body, which a computer reconstructs into detailed cross-sectional images. Modern multidetector CT scanners can produce slices less than one millimetre thick, allowing radiologists to examine the pancreas in fine anatomical detail.
For pancreatic assessment, plain images alone are rarely sufficient. Intravenous iodinated contrast is essential. The contrast highlights the difference between healthy pancreatic tissue, which absorbs contrast readily, and tumour tissue, which typically does not. This difference in enhancement is what makes most pancreatic cancers visible.
The pancreas itself is a flat, elongated gland roughly 15 cm long, divided into the head (nestled in the curve of the duodenum), the body, and the tail (reaching toward the spleen). Roughly 60–70% of pancreatic adenocarcinomas arise in the head of the pancreas, which is fortunate in one respect: head tumours tend to obstruct the bile duct early, causing jaundice and prompting investigation sooner than tumours of the body or tail.
How Does CT Detect Pancreatic Cancer?
The Hypodense Mass
Pancreatic ductal adenocarcinoma — the most common type, accounting for about 90% of pancreatic cancers — is a dense, fibrous tumour with a poor blood supply. When contrast is injected, normal pancreatic tissue lights up brightly while the tumour remains comparatively dark. Radiologists describe this as a hypoattenuating or hypodense mass. This contrast difference is the primary sign of pancreatic cancer on CT.
Secondary Signs
Even when a mass is difficult to see directly, CT often shows indirect clues that point to a tumour:
- Duct dilatation. A blocked pancreatic duct upstream of a tumour becomes dilated. When both the pancreatic duct and the common bile duct are dilated, this is called the “double duct sign” — a finding highly suggestive of a mass in the pancreatic head.
- Abrupt duct cut-off. The pancreatic duct terminates suddenly rather than tapering.
- Distal atrophy. The pancreatic tissue downstream of the obstruction shrinks over time.
- Contour abnormality. A subtle bulge or loss of the normal lobulated pancreatic outline.
- Loss of fat planes. Blurring of the fatty tissue between the pancreas and surrounding vessels.
These secondary signs are the reason experienced radiologists sometimes detect a tumour that is not directly visible as a mass. They are also the findings most often overlooked on a routine scan not specifically designed for the pancreas.
Why Timing Matters: The Pancreatic Protocol
A pancreatic protocol CT — sometimes called a dual-phase or multiphase pancreatic CT — is a specialised technique. Rather than one scan after contrast, images are acquired in two or more distinct phases:
- Pancreatic parenchymal phase (approximately 40–50 seconds after injection). This is when the difference between normal pancreas and tumour is greatest, making this the optimal window for detecting the mass.
- Portal venous phase (approximately 65–80 seconds). This phase is best for assessing liver metastases and venous involvement.
Thin slices, a specific rate of contrast injection, water as a neutral oral contrast agent, and multiplanar reconstructions all form part of the protocol. A standard abdominal CT typically captures only the portal venous phase — which is why small pancreatic tumours can be missed on routine scans.
How Accurate Is CT for Pancreatic Cancer?
This is the question that matters most to patients, and it deserves an honest answer.
Overall detection sensitivity: Pancreatic protocol CT detects approximately 85–95% of pancreatic adenocarcinomas. Specificity is similarly high — when CT shows a mass with classic features, it is usually cancer.
Where accuracy falls: Sensitivity is size-dependent.
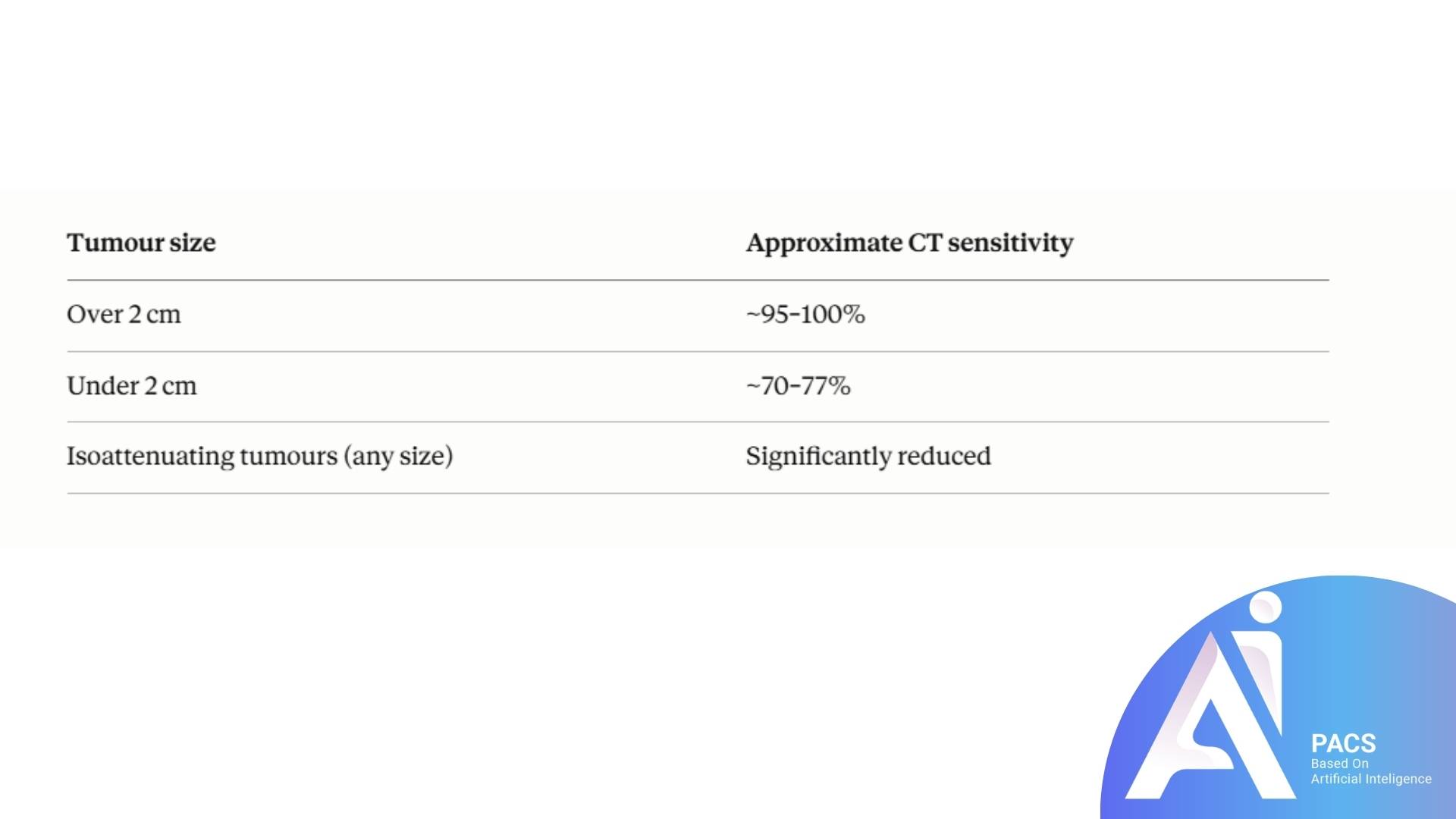
Isoattenuating tumours are a particular challenge. In roughly 5–11% of cases, the tumour enhances at almost exactly the same density as the surrounding pancreas, rendering it essentially invisible as a distinct mass. In these cases, detection depends entirely on the secondary signs described above.
Staging accuracy for resectability — whether the tumour can be surgically removed — is where CT genuinely excels. CT predicts that a tumour is unresectable with an accuracy of around 90–100%. Predicting that a tumour is resectable is somewhat less reliable, at approximately 75–85%, primarily because CT cannot detect microscopic peritoneal deposits or very small liver metastases.
If findings are complex, using AI PACs CT Scan Second Opinion Online Service can provide additional reassurance and expert review.
What CT Can Miss
We believe patients deserve a clear picture of the limits, not only the strengths.
Small tumours. Lesions under 1–2 cm, particularly in the body and tail where there are no early obstructive symptoms, may not be visible.
Isoattenuating lesions. As described above, these blend into normal tissue.
Small liver and peritoneal metastases. Deposits under 5 mm often escape detection. This is one reason some patients are found at surgery to have more advanced disease than CT suggested.
Early cystic precursor lesions. Small intraductal papillary mucinous neoplasms (IPMNs) may be inadequately characterised on CT; MRI with MRCP is superior for these.
Chronic pancreatitis mimics. Inflammatory masses in chronic pancreatitis, and autoimmune pancreatitis in particular, can closely resemble malignancy on CT — and vice versa. Distinguishing them sometimes requires MRI, endoscopic ultrasound, or biopsy.
If your symptoms — persistent upper abdominal or back pain, unexplained weight loss, new-onset diabetes, jaundice, or pale stools — continue despite a normal CT, this warrants further discussion with your physician rather than reassurance alone.
CT Versus Other Imaging Tests
MRI with MRCP
MRI offers superior soft-tissue contrast and is often better for isoattenuating tumours, small liver lesions, and cystic pancreatic lesions. MRCP maps the pancreatic and bile ducts non-invasively. MRI is typically used as a problem-solving tool when CT is inconclusive, or in patients who cannot receive iodinated contrast.
MRI’s soft-tissue strength matters for other abdominal cancers too — for example, whether MRI can detect colon cancer.
Endoscopic Ultrasound (EUS)
EUS places an ultrasound probe directly adjacent to the pancreas via the stomach and duodenum. It has the highest sensitivity for very small tumours — approaching 98% for lesions under 2 cm — and allows fine-needle biopsy in the same session. Its main limitations are operator dependence and its invasive nature.
PET-CT
PET-CT is not a first-line detection tool but is valuable for identifying distant metastases and assessing indeterminate lesions when this would change management.
Transabdominal Ultrasound
Often the first test performed for jaundice or abdominal pain because it is fast and radiation-free. It reliably shows bile duct dilatation but visualises the pancreas poorly in many patients due to overlying bowel gas. A normal abdominal ultrasound does not exclude pancreatic cancer.
Diagnosis and Testing: What to Expect
Before the scan. You will usually be asked to fast for 4–6 hours. Tell the radiology team about kidney problems, diabetes medications (particularly metformin), previous contrast reactions, iodine or shellfish allergy, and any possibility of pregnancy. Blood tests for kidney function are commonly requested.
During the scan. An intravenous cannula is placed, usually in the arm. You may be given water to drink as a neutral oral contrast. The scan itself takes only a few minutes. When contrast is injected, most people experience a brief warm sensation spreading through the body and a metallic taste — this is expected and passes within a minute. You will be asked to hold your breath for short periods.
After the scan. You can return to normal activities immediately. Drinking extra water for the rest of the day helps clear the contrast. Your images are reviewed by a radiologist and a report is issued, typically within one to several days.
Additional tests. CA 19-9 is a blood marker often measured, though it is neither sensitive nor specific enough for diagnosis on its own. Tissue diagnosis, usually via EUS-guided biopsy, is generally required before chemotherapy — though not always before surgery when imaging findings are classic.
How CT Guides Treatment
CT does far more than answer yes or no. Its most consequential role is determining resectability — whether the tumour can be surgically removed, which remains the only route to cure.
Radiologists assess the degree of contact between the tumour and critical vessels: the superior mesenteric artery, coeliac axis, common hepatic artery, superior mesenteric vein, and portal vein. Based on this, tumours are classified as:
- Resectable — no arterial contact, and venous contact of 180° or less without contour irregularity.
- Borderline resectable — limited arterial contact or more extensive venous involvement that may still be reconstructable, often treated with chemotherapy first.
- Locally advanced — arterial encasement beyond thresholds, generally not surgically removable upfront.
- Metastatic — spread to liver, peritoneum, or distant sites.
These distinctions are measured in degrees of vessel circumference and millimetres of contact. They are technically demanding assessments, and interobserver variation is well documented — which is precisely why a specialist second opinion on a pancreatic CT can be decisive.
Practical Tips for Patients
- Ask specifically whether a pancreatic protocol CT was performed. If pancreatic cancer is genuinely suspected and only a routine abdominal CT was done, request the dedicated protocol.
- Obtain your images on CD or via digital transfer, not just the written report. The images are what a second-opinion radiologist needs.
- Keep a symptom diary. Note weight changes, pain patterns, stool colour, and appetite. This information helps your physician judge whether further imaging is warranted.
- New-onset diabetes after age 50 without obvious cause deserves attention, as it can occasionally be the earliest sign of pancreatic cancer.
- Do not accept a single normal scan as final if significant symptoms persist. Repeat imaging after an interval, or a different modality, is sometimes the answer.
- If surgery has been ruled out, consider a second opinion on the vascular assessment. Reclassification from locally advanced to borderline resectable can open the door to potentially curative treatment.
- Stay hydrated and continue eating as well as you are able. Pancreatic enzyme supplements are often helpful if you have fatty stools or unexplained weight loss.
Latest Scientific Findings
Pancreatic protocol CT accuracy (Radiology, 2021). A multi-institutional analysis confirmed that dual-phase pancreatic protocol CT achieved sensitivity above 90% for pancreatic ductal adenocarcinoma overall, but sensitivity dropped substantially for tumours under 2 cm. Significance for patients: the technique used genuinely changes what can be seen — it is reasonable to ask which protocol was performed.
Artificial intelligence in pancreatic CT (Radiology, 2023). A deep-learning model trained on contrast-enhanced CT detected pancreatic cancer with sensitivity comparable to, and in some subgroups exceeding, radiologist performance — particularly for small and isoattenuating lesions. Significance: AI-assisted reading is emerging as a support tool, though it does not yet replace expert human interpretation.
Retrospective review of missed cancers (European Radiology, 2020–2022). Studies reviewing CT scans performed in the months before a pancreatic cancer diagnosis found that a meaningful proportion showed retrospectively visible abnormalities — most often subtle duct dilatation or contour change rather than a frank mass. Significance: this is direct evidence for the value of expert re-review of prior imaging.
Neoadjuvant therapy and CT restaging (Annals of Surgery / JAMA Surgery, 2020–2024). Research on borderline resectable disease showed that CT tends to overestimate residual vascular involvement after chemotherapy — meaning some patients judged inoperable on post-treatment CT are in fact resectable at surgery. Significance: post-chemotherapy CT should be interpreted cautiously and reviewed by a specialist pancreatic team.
MRI as a complement to CT (Abdominal Radiology, 2021–2023). Studies found MRI detected additional small liver metastases in a clinically relevant minority of patients staged as non-metastatic on CT. Significance: MRI may be worth requesting before major surgery.
Note: the studies above are summarised from the published literature in this field; please verify specific citations against the reference list before publication.
Conclusion
So, can a CT scan show pancreatic cancer? In most cases, yes — and when performed as a dedicated pancreatic protocol study and read by an experienced abdominal radiologist, CT remains the cornerstone of both diagnosis and treatment planning. It identifies the tumour, defines its relationship to critical blood vessels, and determines whether surgery is possible.
At the same time, CT is not infallible. Small tumours, isoattenuating lesions, and tiny metastatic deposits can escape detection, and vascular involvement is a genuinely difficult assessment on which experts sometimes disagree.
If you have received a pancreatic CT report and feel uncertain — whether the scan was called normal despite persistent symptoms, or whether you have been told surgery is not an option — a specialist second opinion is a reasonable and often valuable step. Speak with your physician, and consider having your images reviewed by a subspecialist radiologist.