Key Takeaways
- Yes — a CT scan can show a herniated disc, but it is less sensitive than MRI for soft-tissue detail.
- CT excels at bone (facet joints, osteophytes, fractures) and is the first choice when MRI is unavailable or contraindicated (pacemakers, certain implants).
- MRI remains the gold standard for disc herniation, nerve root compression, and spinal cord assessment.
- CT myelography (CT with intrathecal contrast) is highly accurate when MRI cannot be performed.
- Imaging findings must always be correlated with your symptoms — many people have disc bulges on imaging with no pain at all.
What Is a Herniated Disc?
Between each pair of vertebrae sits an intervertebral disc — a cushion with a tough outer ring (the annulus fibrosus) and a soft, gel-like centre (the nucleus pulposus). Think of it as a jam doughnut: firm on the outside, soft in the middle.
A herniated disc occurs when the inner material pushes through a weakened or torn section of the outer ring. If that displaced material presses on a nearby nerve root or the spinal cord, it can cause pain, tingling, weakness, or numbness — often radiating into an arm (cervical herniation) or down a leg (lumbar herniation, commonly called sciatica).
Importantly, not all herniated discs cause symptoms. Studies of asymptomatic adults consistently find disc abnormalities on imaging in people with no back pain whatsoever. This is why a scan result alone never tells the whole story.
Herniation Is Not the Same as a Bulge
Radiologists use precise terms:
- Disc bulge — the disc extends broadly beyond its normal margin (more than 25% of its circumference). Usually a degenerative, age-related change.
- Protrusion — a focal herniation where the base is wider than the displaced material.
- Extrusion — the displaced material is wider than its base; the annulus is fully breached.
- Sequestration — a fragment has separated completely and migrated away from the disc.
These distinctions matter, because they influence prognosis and treatment.
Can a CT Scan Show a Herniated Disc? How CT Actually Works
Yes — and understanding how explains both its strengths and its limits.
A CT (computed tomography) scan uses X-rays taken from many angles around your body. A computer reconstructs these into cross-sectional images. Different tissues absorb X-rays differently, and this absorption is expressed in Hounsfield units.
Here is the crux: bone absorbs X-rays strongly and appears bright white. Air appears black. But the soft tissues of the spine — the disc, the nerve roots, the thecal sac, the ligaments — all have similar X-ray absorption. On CT, they appear in narrow, closely-spaced shades of grey.
So a CT scan can show a herniated disc when the displaced disc material creates enough contrast against the surrounding epidural fat or the thecal sac. Herniations that are large, calcified, or that indent the theca are often clearly visible. Small, soft, or laterally-positioned herniations may be far harder to appreciate.
If findings are complex, using AI PACs CT Scan Second Opinion Online Service can provide additional reassurance and expert review.
What CT Sees Very Well
- Vertebral fractures and bony injury
- Osteophytes (bone spurs) narrowing the neural foramen
- Facet joint arthropathy
- Spinal canal dimensions and bony stenosis
- Calcified disc herniations
- Post-surgical hardware, screws, and cages
- Spondylolysis (pars defects)
What CT Sees Less Well
- The spinal cord itself and any cord signal change
- Individual nerve roots and their compression
- Disc hydration and early degeneration
- Annular tears
- Inflammation, oedema, and infection
- Distinguishing recurrent disc herniation from post-operative scar tissue (without contrast)
CT vs MRI for Herniated Disc — Which Is Better?
MRI is the gold standard. There is broad consensus on this across radiology and spine surgery. The American College of Radiology Appropriateness Criteria rate MRI without contrast as the most appropriate initial advanced imaging for suspected lumbar disc herniation with radiculopathy.
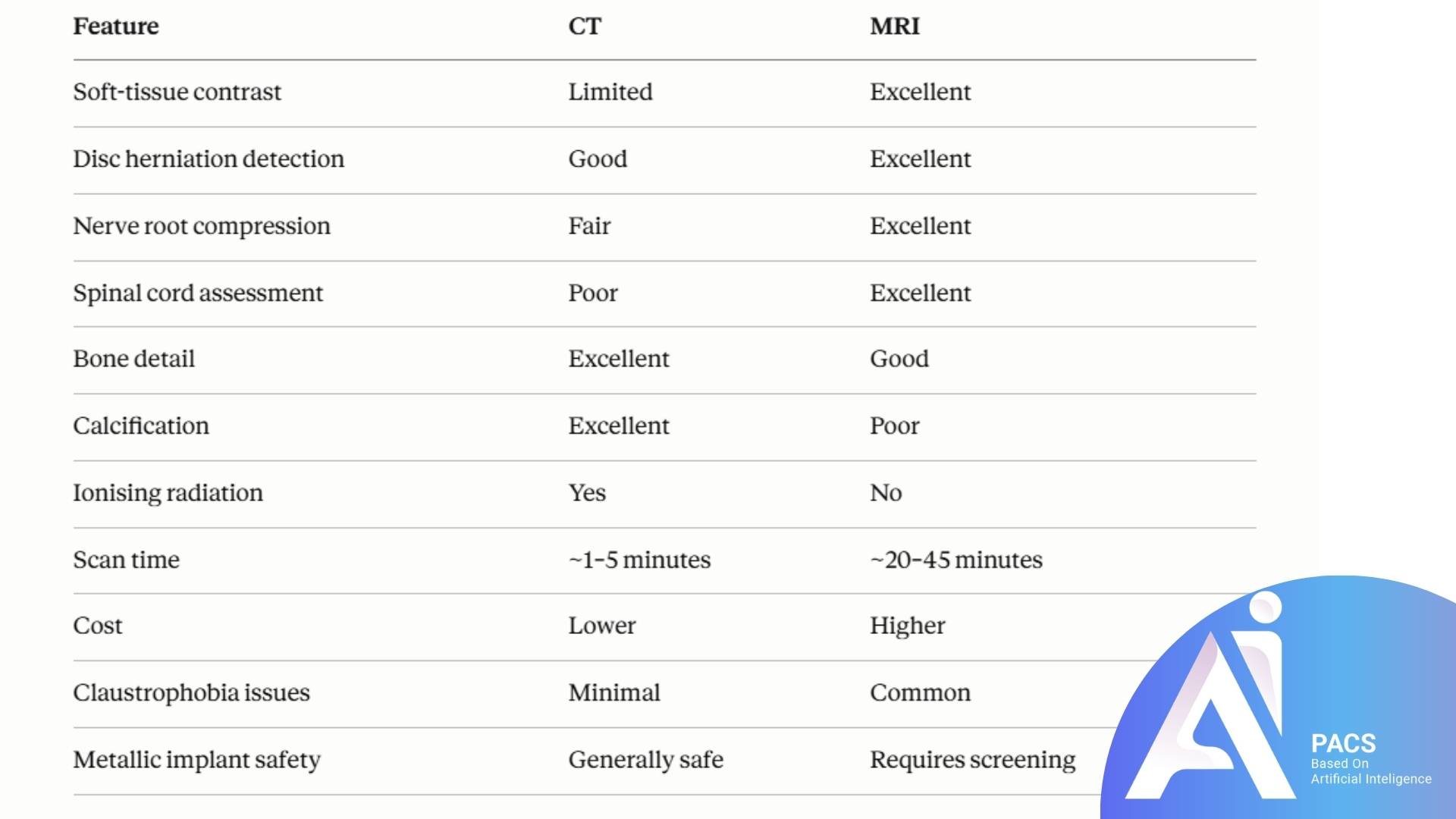
MRI’s advantage comes from its ability to distinguish tissues by their water and fat content rather than their density. On a T2-weighted MRI, cerebrospinal fluid appears bright, making a dark disc fragment pressing into it immediately obvious. It can also show whether a nerve root is genuinely compressed, displaced, or merely abutted — a distinction with real surgical consequences.
So Why Would Anyone Order a CT?
There are entirely legitimate reasons:
- MRI is contraindicated. Certain pacemakers, cochlear implants, some aneurysm clips, and retained metallic foreign bodies in the eye may make MRI unsafe.
- The patient cannot tolerate MRI. Severe claustrophobia or an inability to lie still for 30+ minutes.
- Speed matters. In trauma, CT is fast and rules out fracture immediately.
- Bone is the primary question. If the clinical concern is bony stenosis or a pars defect, CT may be more informative.
- Surgical planning. Spine surgeons often want CT alongside MRI to assess bone quality and calcification.
- Availability and cost. In many regions, CT is more accessible and affordable.
CT Myelography — The High-Accuracy Alternative
When MRI truly cannot be performed but detailed nerve information is essential, CT myelography is the answer.
A radiologist injects iodinated contrast into the cerebrospinal fluid via a lumbar puncture. The contrast fills the thecal sac and outlines the nerve roots. A CT is then performed. Any disc herniation indenting the theca now appears as a sharp, unmistakable filling defect.
CT myelography approaches MRI in accuracy for detecting disc herniation and nerve root compression. It is, however, an invasive test carrying small risks: post-procedural headache, infection, contrast reaction, and radiation exposure. For this reason it is reserved for patients in whom MRI is not an option, or where MRI findings are equivocal and surgery is being planned.
Symptoms That Prompt Imaging
You do not need a scan for every episode of back pain. Most acute back pain improves within 4–6 weeks with conservative care, and imaging in the first six weeks — absent red flags — often leads to unnecessary intervention without improving outcomes.
Imaging is appropriate when:
- Radicular pain (sciatica, or arm pain from the neck) persists beyond 4–6 weeks despite conservative treatment
- Progressive neurological deficit — worsening weakness, foot drop, loss of reflexes
- Surgery or injection is being actively considered
Seek urgent medical attention — do not wait — if you experience:
- Loss of bladder or bowel control
- Numbness in the saddle region (inner thighs, buttocks, genitals)
- Rapidly progressive leg weakness in both legs
- Severe pain with fever, unexplained weight loss, or a history of cancer
These may indicate cauda equina syndrome or another serious condition requiring emergency assessment.
What to Expect During a Spine CT
Preparation is minimal, which is one of CT’s practical advantages.
Before: You will usually eat and drink normally unless contrast is planned. Remove metal objects — belts, jewellery, coins. Tell the radiographer if you are or might be pregnant.
During: You lie on your back on a table that moves through a large ring-shaped scanner. It is open at both ends, so claustrophobia is rarely a problem. The scan itself typically takes less than a minute of actual imaging. You will be asked to hold still, and sometimes to hold your breath briefly.
After: There are no after-effects. You may drive and return to normal activity immediately. If contrast was used intravenously, you will be asked to drink extra fluids.
Radiation: A lumbar spine CT delivers a meaningful radiation dose — roughly equivalent to several years of natural background radiation. This is not a reason to refuse a clinically indicated scan, but it is a reason not to have one unnecessarily.
Treatment Options for a Herniated Disc
Reassuringly, the natural history of disc herniation is largely favourable. Most herniated discs improve without surgery — and many actually shrink over time as the body resorbs the displaced material.
Conservative Management (First-Line)
- Relative rest, then movement. Prolonged bed rest is counterproductive. Gentle activity is encouraged.
- Physical therapy. Core strengthening, directional preference exercises, and graded activity.
- Analgesia. NSAIDs, paracetamol; neuropathic agents in selected cases.
- Education and reassurance. Understanding that pain does not equal damage genuinely improves outcomes.
Interventional Options
- Epidural steroid injection. Can provide meaningful short-to-medium-term relief of radicular pain, often used as a bridge while natural resolution occurs.
- Nerve root block. Both diagnostic and therapeutic.
Surgery
- Microdiscectomy. Removal of the herniated fragment through a small incision. Considered for persistent radicular pain beyond 6–12 weeks, or earlier with progressive weakness.
- Emergency decompression. Mandatory for cauda equina syndrome.
Surgery tends to deliver faster relief than conservative care, though the difference in outcomes narrows considerably at one to two years. It is a decision about timing and preference as much as necessity, in the absence of red flags.
Practical Tips for Patients
- Bring your images, not just the report. If you seek a second opinion, the DICOM images matter far more than the written summary.
- Ask which test is right for your question. If your CT was ordered for trauma, it may not have been optimised for disc assessment.
- Don’t be alarmed by the word “degenerative.” It appears on the majority of adult spine reports and is often the radiological equivalent of grey hair.
- Correlate with symptoms. A left-sided herniation should not be blamed for right-sided pain. If your imaging and symptoms don’t match, say so.
- Keep moving. Deconditioning worsens outcomes.
- Avoid repeat imaging without a change in symptoms. Serial scans rarely change management.
Latest Scientific Findings
1. Asymptomatic findings are the norm (Brinjikji et al., AJNR, 2015). This landmark systematic review found disc degeneration in 37% of 20-year-olds and 96% of 80-year-olds without symptoms. Disc protrusion was present in 29% of asymptomatic 20-year-olds. What this means for you: finding a herniated disc on any scan does not automatically explain your pain.
2. Spontaneous resorption is common (Zhong et al., Pain Physician, 2017; Chiu et al., Clinical Rehabilitation, 2015). Meta-analyses report spontaneous regression rates of roughly 66–96% depending on herniation type — with sequestrated fragments resorbing most readily. What this means for you: time is genuinely a treatment.
3. Early imaging does not improve outcomes (Chou et al., Lancet; ACP Guidelines, 2017). Routine imaging for acute low back pain without red flags shows no benefit in pain or function, and is associated with higher costs and more surgery. What this means for you: your physician declining a scan may be good medicine, not neglect.
4. MRI outperforms CT for disc and nerve assessment. Comparative studies and ACR Appropriateness Criteria consistently rank MRI as superior for soft-tissue and neural evaluation, while confirming CT’s superiority for bony detail. What this means for you: the “best” scan depends on the question.
5. CT myelography remains highly accurate. Where MRI is contraindicated, CT myelography demonstrates diagnostic accuracy comparable to MRI for surgically relevant disc herniation. What this means for you: a pacemaker does not mean you cannot be properly diagnosed.
Conclusion
So — can a CT scan show a herniated disc? Yes, it can, and in many cases it does so clearly. But CT is not the ideal tool for the job. It was built to see bone, and it sees bone brilliantly. Discs, nerve roots, and the spinal cord are better served by MRI, which is why MRI remains the standard of care for suspected disc herniation.
If you have already had a CT and remain uncertain about the findings, that uncertainty is worth addressing. A subspecialist radiologist reviewing your original images — not just the report — can often clarify whether what was seen truly explains your symptoms, and whether further imaging is warranted.
Most herniated discs get better. Understanding your imaging is the first step in getting better with confidence rather than anxiety.
Scientific References
- Brinjikji W, Luetmer PH, Comstock B, et al. Systematic Literature Review of Imaging Features of Spinal Degeneration in Asymptomatic Populations. AJNR Am J Neuroradiol. 2015;36(4):811–816. DOI: 10.3174/ajnr.A4173
- Qaseem A, Wilt TJ, McLean RM, Forciea MA. Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Ann Intern Med. 2017;166(7):514–530. DOI: 10.7326/M16-2367
- Chou R, Fu R, Carrino JA, Deyo RA. Imaging strategies for low-back pain: systematic review and meta-analysis. Lancet. 2009;373(9662):463–472. DOI: 10.1016/S0140-6736(09)60172-0
- Zhong M, Liu JT, Jiang H, et al. Incidence of Spontaneous Resorption of Lumbar Disc Herniation: A Meta-Analysis. Pain Physician. 2017;20(1):E45–E52.
- Chiu CC, Chuang TY, Chang KH, et al. The probability of spontaneous regression of lumbar herniated disc: a systematic review. Clin Rehabil. 2015;29(2):184–195. DOI: 10.1177/0269215514540919
- American College of Radiology. ACR Appropriateness Criteria® Low Back Pain. ACR, 2021. https://acsearch.acr.org/docs/69483/Narrative/
- Fardon DF, Williams AL, Dohring EJ, et al. Lumbar disc nomenclature: version 2.0. Spine J. 2014;14(11):2525–2545. DOI: 10.1016/j.spinee.2014.04.022
- Weber H. Lumbar disc herniation: a controlled, prospective study with ten years of observation. Spine. 1983;8(2):131–140.
- Peul WC, van Houwelingen HC, van den Hout WB, et al. Surgery versus prolonged conservative treatment for sciatica. N Engl J Med. 2007;356(22):2245–2256. DOI: 10.1056/NEJMoa064039
- RadiologyInfo.org. Computed Tomography (CT) – Spine. Radiological Society of North America. https://www.radiologyinfo.org/en/info/ct-spine
- Mayo Clinic. Herniated disk – Diagnosis and treatment. https://www.mayoclinic.org/diseases-conditions/herniated-disk/diagnosis-treatment/drc-20354101
- Cleveland Clinic. Herniated Disk. https://my.clevelandclinic.org/health/diseases/12768-herniated-disk
This article is educational and does not replace assessment by a qualified physician.